

Understanding Acid-Base Imbalances: A Simple Guide for Nurses
Introduction
Acid-base imbalances are one of those topics that can feel overwhelming at first. Between pH, PaCO₂, HCO₃, and compensation, it’s easy to get lost in the numbers. But here’s the truth: You don’t need to memorize everything to understand it. You just need a clear framework.
Whether you’re a nursing student, new grad, or transitioning into a higher-acuity setting, this guide will help you simplify acid-base interpretation and start thinking through it with confidence.
Why Acid-Base Balance Matters
Your patient’s acid-base status gives you rapid insight into what’s happening internally.
It can signal:
Respiratory failure
Kidney dysfunction
Sepsis
Medication effects
Shock states
In high-acuity settings like the ER, recognizing these patterns early can change outcomes.
The Basics You Need to Know
Let’s break it down into the essentials:
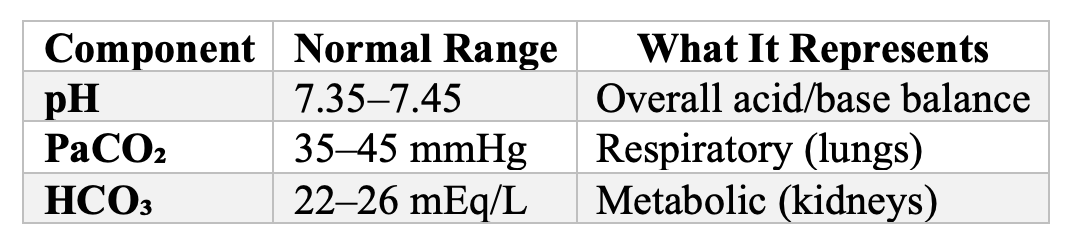
Acid-Base Components and Normal Ranges
Step-by-Step ABG Interpretation (Keep It Simple)
Instead of overcomplicating it, use this 3-step approach:
Step 1: Look at the pH
< 7.35 → Acidosis
>7.45 → Alkalosis
Step 2: Determine the Primary Cause
PaCO₂ abnormal → Respiratory issue
HCO₃ abnormal → Metabolic issue
Step 3: Check for Compensation
Is the other system trying to correct it?
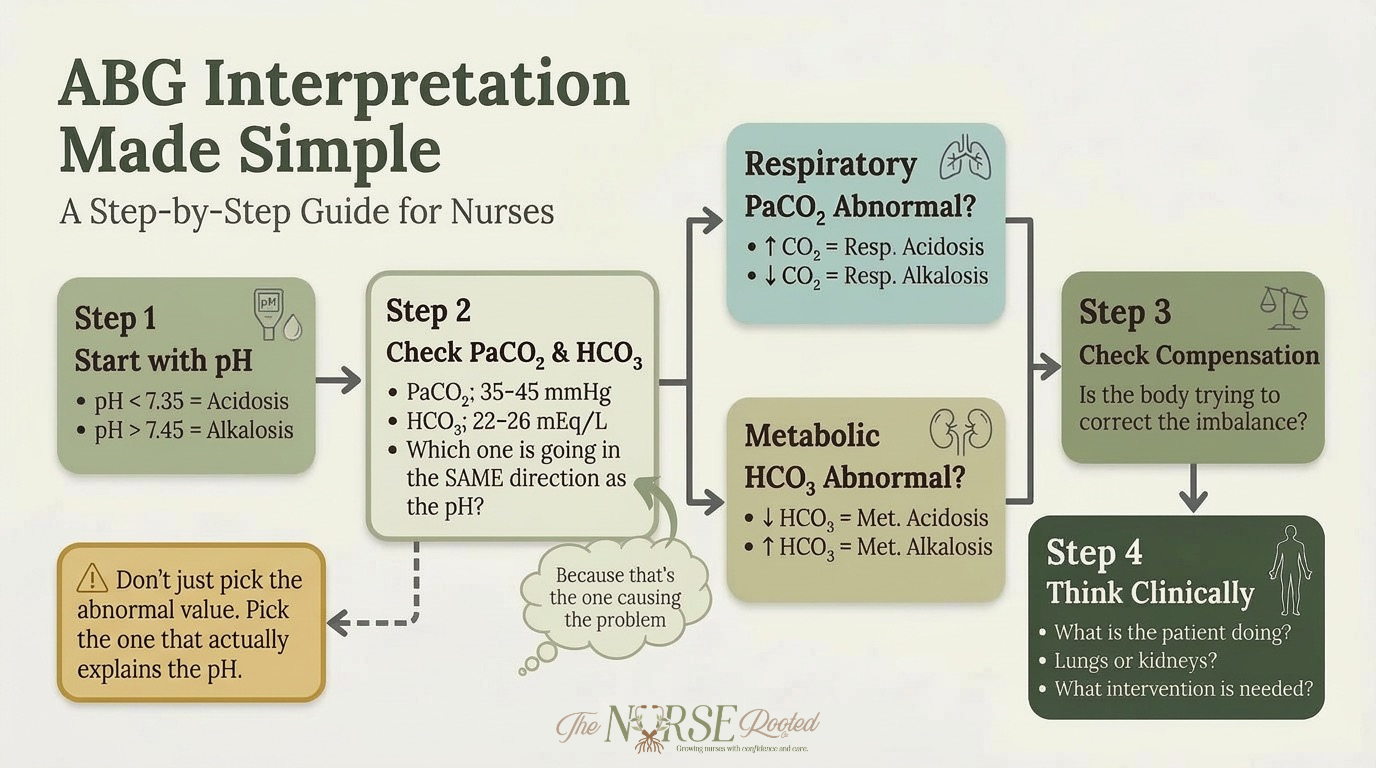
ABG Interpretation Made Simple
The Four Primary Imbalances
1. Respiratory Acidosis
Cause: Hypoventilation
CO₂ increases → pH decreases
Common causes:
COPD
Sedation/opioids
Airway obstruction
2. Respiratory Alkalosis
Cause: Hyperventilation
CO₂ decreases → pH increases
Common causes:
Anxiety
Pain
Early sepsis
3. Metabolic Acidosis
Cause: Decreased HCO₃ or increased acid
Common causes:
DKA
Renal failure
Severe diarrhea
4. Metabolic Alkalosis
Cause: Increased HCO₃
Common causes:
Vomiting
NG suction
Diuretics
Quick Reference Table (Save This!)
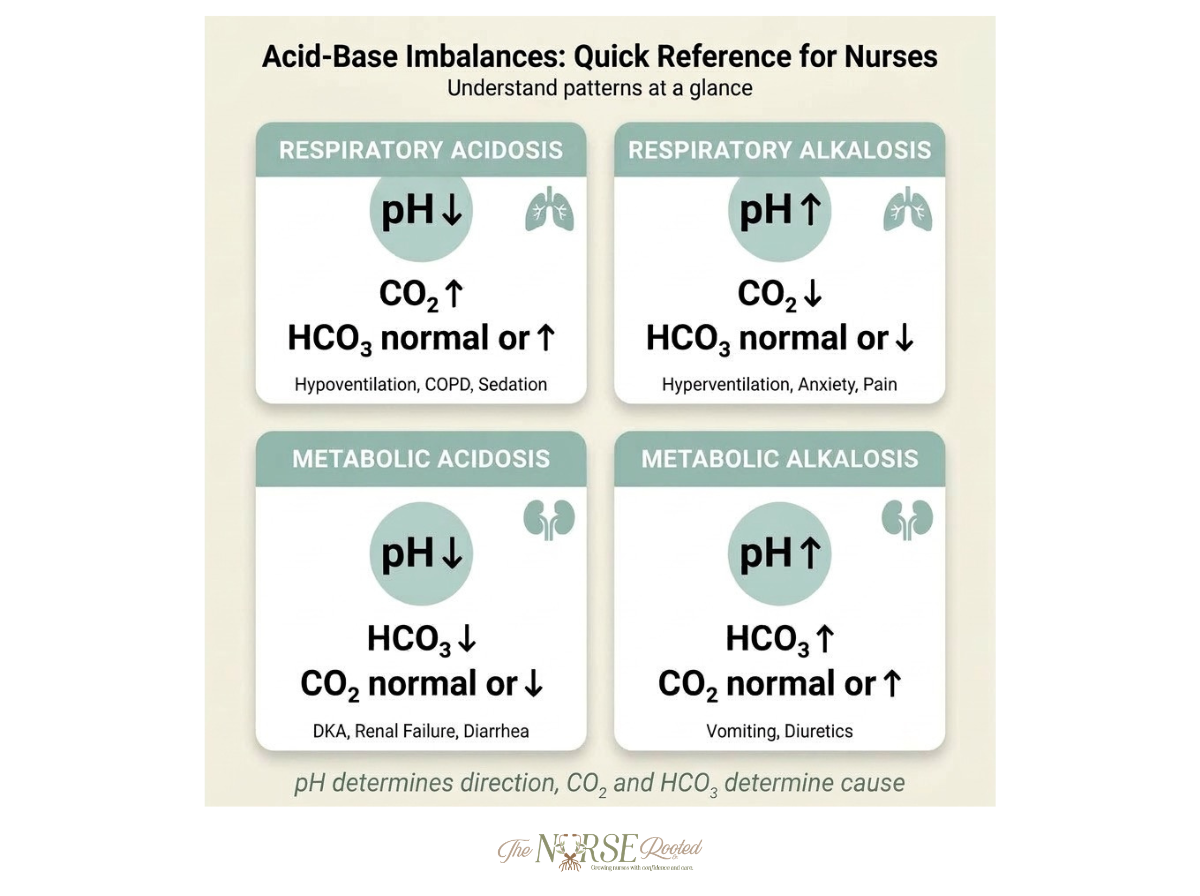
Acid-Base Imbalances: Quick Reference Table
Clinical Application: What This Looks Like in Real Life
Let’s bring this to the bedside.
You receive an ABG:
pH: 7.30
PaCO₂: 50
HCO₃: 24
What does this tell you?
pH is low → Acidosis
CO₂ is high → Respiratory cause
HCO₃ is normal → No compensation yet
Interpretation: Respiratory Acidosis
Now your brain shifts from memorization to clinical thinking:
Is the patient hypoventilating?
Do they need airway support?
Are they on opioids or sedatives?
That’s where confidence starts to build.
Pro Tips for Nurses
Don’t try to memorize everything. Focus on patterns.
Always start with pH first
Think lungs vs kidneys
Connect values to what’s happening in the patient
Practice with real cases as often as possible
Bringing It All Together
Acid-base imbalances aren’t about complicated equations. They’re about understanding what the body is trying to tell you. When you approach ABGs with a structured method, you move from “I have no idea what this means” to “I can figure this out step by step.” And that’s where real clinical confidence begins.
Disclaimer
The content provided by The Nurse Rooted Co. is intended for educational and informational purposes only. It is not a substitute for professional medical advice, clinical judgment, nursing supervision, or legal consultation. All users are responsible for ensuring that any actions taken based on this content are within their legal scope of practice and comply with their employer's policies and procedures, the state board of nursing's policies, and applicable laws. The Nurse Rooted Co. does not provide medical care, legal services, or employment supervision. Use of this content does not establish a nurse-client or mentor-client relationship unless explicitly agreed upon through a signed mentorship agreement. By accessing or using this content, you agree to use it responsibly and understand that The Nurse Rooted Co. is not liable for decisions or actions taken based on this material.